Got aches and pains? We’ve got Kristen DeStefano, our physical therapist, to the rescue! Today she talks about one of the climber problems: elbow Injury, and how to deal with ’em.
The outdoor climbing season is in full swing now, and you’ve been getting after it every week with gym sessions, hang board routines, and campus boarding in between. What you might not realize is these repetitive and high-stress movements are a killer on your elbows. When it comes to climbing, whether you are a lifer or a top rope hero (What Kind of Climber Are You?), chances are your elbows are going to start to ache at some point in your career. Don’t worry! You’re not doomed. Here’s what could be going on.
Check out our post on training from home, here!!!

Courtney Sanders putting those elbows to the test.
Elbow Injury Lists In Common Climber Problems
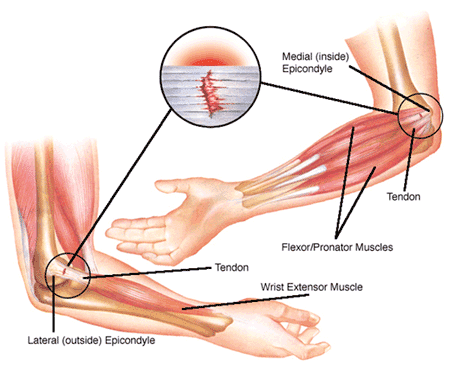
The elbow is a joint made up of the lower part of the humerus and the upper ends of the ulnar and radius, which make up the forearm. Four movements can occur at this joint. They are flexion (bending the elbow), extension (straightening the elbow), supination (turning the palm up), and pronation (turning the palm down). At the lower end of the humerus, you will see two bony prominences on either side. These are called the medial epicondyle (on the inside) and the lateral epicondyle (on the outside). These areas serve as muscle attachment sites, and therefore can be common spots for injury, particularly in climbers.

The Dreaded “Epicondylitis”
Epicondylitis (a blanket term that includes tennis and golfer elbows) is a disorder widely regarded as a type of tendinitis, which literally means “inflammation of the tendon”. As most everyone knows, inflammation is best handled with NSAIDs (like Advil) and ice. End of story, right? Not really… which may explain why so many climbers have chronic elbow problems that aren’t cured with ice and NSAIDs.
Recent research strongly suggests that inflammation is rarely found in epicondylitis other than briefly during the earliest stages. Since it’s probably an error to describe these conditions as “itis” (i.e. swelling), many clinicians now referring to these conditions as tendinopathies, which are painful conditions occurring in tendons in response to overuse. Sound familiar? Therefore, it is now believed that epicondylitis is a degenerative disorder caused by chronic tendon exhaustion and muscle irritation in the elbow which can affect both the outside (lateral) and the inside (medial) of the elbow. So which do you have? Read on to find out.
“Tennis Elbow” (Lateral Epicondylitis)
On the outside of the elbow, a common tendon of the wrist extensors and supinator muscles attaches to the bone. These muscles are responsible for opening up your hand, bending your hand backward, and rotating your palm upward. This is called lateral epicondylitis, which is also known as “tennis elbow”.
Lateral epicondylitis has a 9:1 incidence ratio when compared to its cousin medial epicondylitis. When pain occurs here, you will likely have pain when using pinches, crimps, and underclings, or even with activities as simple as holding your coffee cup or turning a door knob. Pain may also radiate down the outside of your forearm. Unfortunately, tennis elbow most commonly affects men and those between 35 to 50 years of age. Sorry guys!
“Golfer’s Elbow” (Medial Epicondylitis)
Medial epicondylitis, also known as “golfer’s elbow” is an irritation to the attachment of the wrist flexors and pronators on the inside of the elbow. These muscles close your hand into a fist, bring your palm towards your forearm, and rotate your palm downward. Unlike the outside of the elbow, there appears to be an equal prevalence between men and women, with most cases reported in the dominant arm.
So, How Do I Fix it?
Rest
As epicondylitis is caused by chronic tendon exhaustion, rest is the first line of defense to resolve this condition. As this is the “boring” treatment option many people ignore or half-heartedly comply with this recommendation. If pain persists for longer periods more rest will likely be required to resolve the pain.
Ice
At the first sign of elbow pain your best bet is to use ice. Ice helps to reduce inflammation and is also a good analgesic to numb pain. As previously discussed, when epicondylitis is in its chronic phases irritation is caused by degeneration and not inflammation, and therefore ice may have little effect besides it’s analgesic benefits. One common method of icing is ice massage. To perform ice massage, fill a small dixie cup with water and freeze it.
Once frozen, rip the cup to expose the ice. Move the ice in circular motions around the painful area for about 10 minutes. As the ice melts, tear down the sides of the cup further to further expose the ice. When in a pinch, you can always resort to using an ice pack or the trusty bag of peas over the affected area for about 15 minutes.

Self Massage
Again, due to the chronicity of epicondylitis, muscle tension and tightness frequently exacerbates this condition. Massage can help to alleviate this tension. Use firm long strokes from mid-forearm to elbow along the muscle. Applying lotion can help to reduce irritation of the skin. Pressure should be firm, like that used to wring out a sponge.
Stretching
Stretching can be helpful to combat muscle tightness and spasm in the forearm musculature. To stretch the extensors on the lateral epicondyle, straighten your elbow and use your other hand to bend your wrist downward. To make the stretch more intense, rotate the forearm so the thumb points downward to the floor. To stretch the wrist flexors on the medial epicondyle, straighten the elbow and use your other hand to bend the wrist upward and the fingers back. Stretches can be held for 30 to 60 seconds and should be performed three times.

Wrist Extensor Stretch for Lateral Epicondylitis

Wrist Flexor Stretch for Medial Epicondylitis
Strengthening
Eccentrics (negatives), or a slow-releasing of a muscle contraction, are frequently used for the rehabilitation of tendon related disorders. It is believed that the tension created by eccentric contractions forms new fibrous tissue at the junction between the muscle and the tendon, making it more resistant to damage. Start with a low level weight (2-3 lb dumbbell). Sit next to a table with your elbow bent to 90 degrees and your hand hanging over the edge of the table.
Use your other hand to elevate the weighted hand then slowly lower back to the starting position. I personally recommended using a count of 5 seconds to lower the weight to prevent from performing them too quickly. Complete 10 repetitions, then rest. You can do two to three sets of these. Be aware that there may be some pain noted with this exercise. It should be tolerable, and only felt while exercising. “Bad pain” is noted by an increase in symptoms later that day or the next day.
If this is experienced, you should cut back on the amount of weight or the number of repetitions performed. As the exercises becomes easier and there is little to no pain, you can progress the regimen by increase the weight by one to two pounds or by decreasing the amount of bend in the elbow.
Click here for descriptions for each exercise. And, before you get started, one thing to note, you may find it beneficial to strengthen all the muscles of your forearm, however for lateral epicondylitis you will get the best results with focus on wrist extension, radial deviation, and supination. For medial epicondylitis wrist flexion, ulnar deviation, and pronation should be emphasized. In persistent cases it may take 4 to 6 weeks to fully recover using these exercises.

Steph Davis throwin’ bows.
Now That You’re Rehabilitated… How To Prepare For Redpoint Attempts
So you’ve fallen off your project for the fifth or sixth time now and your back with both feet on the ground wondering what you should do next. Your forearms might be burning, but you aren’t overly pumped, and your elbow pain (if you have it) is pretty calm. Here are some helpful tips to maximize your performance to get the send and give those elbows and the rest of your body the love they deserve.
Warm Up
A proper warm up is essential to any physical activity, particularly when it is a maximum effort. Start with a climb that is a few grades below that of the one you’re projecting. If you are looking to red point a 5.12a, start your warm up with a 5.10c to loosen up your muscles and get the blood flowing. Try a couple other climbs with lower grades as well. Also consider if your climb is very technical and full of crimps it would be in your best interest to warm up on a climb that includes crimps as opposed to a dynamic overhung jug haul.
Rest
It’s the second time I’ve mentioned rest, and it’s the second time you’re rolling your eyes. I know, I know, it seems like wasted time but in the long run it will give your body some time to regroup in between burns. How long do you rest? For maximum recovery, research has supported a minimum 5:1 rest to work ratio. This means if your working your problem for thirty seconds before popping off two and a half minutes of rest is recommended, on for one minute then rest for five, so on and so forth.
That being said, intensity of the climb can vary and climbers may even benefit from rests upwards of 10 to 15 minutes in between full effort burns. Rapid fire trials will only increase forearm pump and make you more prone to injury, not to mention decrease the likelihood of sending.
Nutrition
While you’re taking time to rest, this is the perfect opportunity to refuel. Carbohydrates and protein are essential to athletic performance and recovery. The consumption of carb during long bouts of high intensity activity can help to quickly replenish your body’s energy stores. Carbs are classically made up of simple sugars which are digested quickly and then pumped through your blood to your muscles for energy. Fruits (yes, fruits have carbs) can be particularly good at this. Try fruits such as bananas, oranges, or grapes (raisins, too). Staying hydrated with water or drinks such as gatorade will combat muscle fatigue, cramps, and keep your muscles flexible.
Stretching
Contrary to common belief, static stretching (holding a stretch for 30 seconds or greater) DURING performance may actually be counterproductive. Static stretching is essential to maintaining healthy muscle tissue and tissue length but should be used post activity to help recovery. Dynamic stretching, or stretching through movement, can help to increase blood flow to the target muscle, maintain range of motion, and increase athletic performance. To perform dynamic stretching, move into the maximum range of motion with a slow and controlled motion. A stretch should be felt at end range.
For your wrists, you can use a slow motion of pumping your wrists and fingers back and forth with your elbows straight to loosen up your forearms. Dynamic stretching can be most beneficial during your warm up routine.
Stay strong and climb on!
-Kristen
If you have more aches and pains, check out Kristen’s past posts on shoulders and fingers! And if you have a request for a future post, leave a comment below, or send us an email to let us know!
Photo Credits (in order): Lifesportchiro.com, WebMD, badmintoncentral.com, Cryocup.com,hep2go.com, highinfatuation.com





